Hypertension Guideline 2018 ไทย
5 เดือน)
- ก่อนที่จะมีการพัฒนาใช้ anti-hypertensive medication: 7% ของผู้ป่วย Hypertension ทั้งหมด จะพบภาวะ Hypertensive Emergencies
- ปัจจุบันลดลงเหลือเพียง 1-2%
- The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (latest 2003)
- ไม่ระบุใน JNC 7
- Systolic BP >=180 หรือ Diastolic BP >=110 mmHg ควรระวังภาวะ HTE 1
- End-organ damage มักพบเมื่อ SBP >220, DBP > 120 2
- Report of JNC 1993 ได้กำหนด
- Hypertensive crises = HT Emergencies + HT Urgencies
- ในปัจจุบัน กำหนดให้ดูที่ evidence of acute target-organ damage
- ถ้ามี … = HT emergency = Rx ลดความดันภายในระยะเวลาเป็น " ชั่วโมง "
- ถ้าไม่มี.. =HT urgency = Rx ลดความดันภายใน 24-48 ชั่วโมง
Ref: CHEST 2007; 131: 1949-1962: Hypertensive crises: challenges and management HT Emergency HT Urgency End-organ damage มี ไม่มี ความเร่งรีบในการลดความดัน ชั่วโมง วัน ประเภทยาลดความดันที่ใช้ Parenteral oral 13. JNC 7 th
- Malignant Hypertension:
- เคยถูกใช้เพื่อบรรยาย HT with encephalopathy, or acute nephropathy.
- แต่ต่อมาถูกถอนออกจาก National and International Blood Pressure Control guideline
- ซักประวัติ มองหา sign of target-organ damage หากมี มักเป็นอาการสำคัญที่พาผู้ป่วยมาโรงพยาบาล ไม่ค่อยมีปัญหาในการ detect
- ในขณะที่ผู้ป่วยที่ไม่มีอาการ (Clinical stable) จะมีภาวะดังต่อไปนี้ที่อาจทำให้ BP สูงขึ้นได้ ต้องซักประวัติเพื่อ rules out.
- Anxiety
- Pain
- การใช้สารกระตุ้น sympatomimetic drug เช่น amphetamine, cocaine, phencyclidine
- อยู่ในภาวะขาดสุรา withdrawal state of alcohol
- อยู่ในภาวะ ขาดยา หรือไม่ได้กินยา Hypertension
Successfully reported this slideshow. พ. ญ. นลินาสน์ ขุนคล้าย Working at Thai Association for Emergency Medicine 1. Hypertensive Emergencies and Urgencies Nalinas Khunkhlai, MD Department of Emergency Medicine Rajavithi Hospital 2. case
- หญิง 56 ปี โรคไต (CKD) มาที่ ER ด้วยอาการเพลีย เวียนศีรษะบ้านไม่หมุน BP220/110 รู้สึกตัวดี ไม่ซีด ท่านจะให้การรักษาแบบ
- Admit ICU
- IV nicardipine
- IV NTG
- Observe ขอดูไปก่อน
- None of above
- 2. ชาย 55 ปี บ่นปวดศีรษะแล้วหมดสติบนแท้กซี่ก่อนถึงรพ. Lt. hemiparesis. BP 240/100
- Admit ICU
- IV nicardipine
- IV metoprolol
- Observe
- None of above
- 3. ชาย 54 ปี เพิ่งกลับจากจ้อกกิ้ง แวะมา 7-11 ในรพ. แล้วรู้สึกตามัว จึงมาตรวจที่ ER BP 270/135 X0#@/
- Admit ICU
- เจาะเลือดซะเลย
- IV metoprolol
- Observe
- None of above
- 4.
แล้วรู้สึกตามัว จึงมาตรวจที่ ER BP 270/135 X0#@/
- Admit ICU
- เจาะเลือดซะเลย
- IV metoprolol
- Observe
- None of above
- 4. ชาย 66 ปี heavy smoking เจ็บแน่นหน้าอกทันที BP 245/130 เจ็บมากกกกก เหมือนโดนฉีกอก
- Admit ICU
- เจาะเลือดซะเลย
- ตาม หมอโรคหัวใจ
- Observe
- None of above
ตรวจร่างกาย และตรวจพิเศษ
- มองหา end-organ damage ตามระบบ หา new s/s ที่มีความสัมพันธ์กับภาวะความดันโลหิตสูง
- Pulse 4 extremities. ( detect dissecting)
- CXR มองหา
- Sign of volume overload ( Heart faiure)
- Thoracic aortic dissecion
- Clue = chest pain + High BP
- ความดันที่สูงจะยิ่งทำให้เกิดการเซาะของผนังหลอดเลือด และก่อให้เกิดอันตรายมากขึ้น
- แนวทางการรักษา: ลด LVEF เพื่อลด flow velocity และลดอาการบาดเจ็บของเส้นเลือด
ชาย 66 ปี heavy smoking เจ็บแน่นหน้าอกทันที BP 245/130 เจ็บมากกกกก เหมือนโดนฉีกอก
- Admit ICU
- เจาะเลือดซะเลย
- ตาม หมอโรคหัวใจ
- Observe
- None of above
- Hypertensive crisis
- Hypertensive emergencies
- Hypertensive urgencies
- รายงานและตีพิมพ์ครั้งแรกโดย Volhard and Fahr 1 ในปี 1914
- ผู้ป่วยมีอาการแสดงของ severe HT + sign of vascular injury to heart, brain, retina, kidney.
- อาการดังกล่าวเกิดขึ้นอย่างรวดเร็ว, rapid fatal course. End up with heart attack, renal failure, stroke.
- 1939: 1 st large study of the natural history of Hypertensive emergencies.
- ผลการศึกษา: Untreated Hypertensive Emergencies มี 1-yr mortality rate 79% ( อายุขัยเฉลี่ย 10.
- กรุงเทพ - ไคสี จ.บึงกาฬ - จองตั๋วรถทัวร์ ระบบออนไลน์
- สูตร น้ำยา ลาว hd
- Hypertension guideline 2018 ไทย full
- Hypertension guideline 2018 ไทย pdf
- Hypertension guideline 2018 ไทย เต็มเรื่อง
- Hypertension guideline 2018 ไทย free
- ศูนย์การศึกษาต่อเนื่องทางเภสัชศาสตร์
- บ รี ส สีชมพู หมายถึง
Stroke
- กรณีที่มักเป็นกังวล = intracranial hematoma
- No evidence that hypertension provoke further bleeding
- มีรายงานว่า SBP >200, DBP>110, MABP>130 จึงค่อยเริ่มควบคุมความดัน แต่ไม่ต้องให้ลดลงอย่างเร็วมาก
- ลดเร็ว พบว่า increase 24hr. mortality
- หญิง 56 ปี โรคไต (CKD) มาที่ ER ด้วยอาการเพลีย เวียนศีรษะบ้านไม่หมุน BP220/110 รู้สึกตัวดี ไม่ซีด ท่านจะให้การรักษาแบบ
- Admit ICU
- IV nicardipine
- IV NTG
- Observe ขอดูไปก่อน
- None of above
- 2. BP 240/100
- Admit ICU
- IV nicardipine
- IV metoprolol
- Observe
- None of above
- 3.
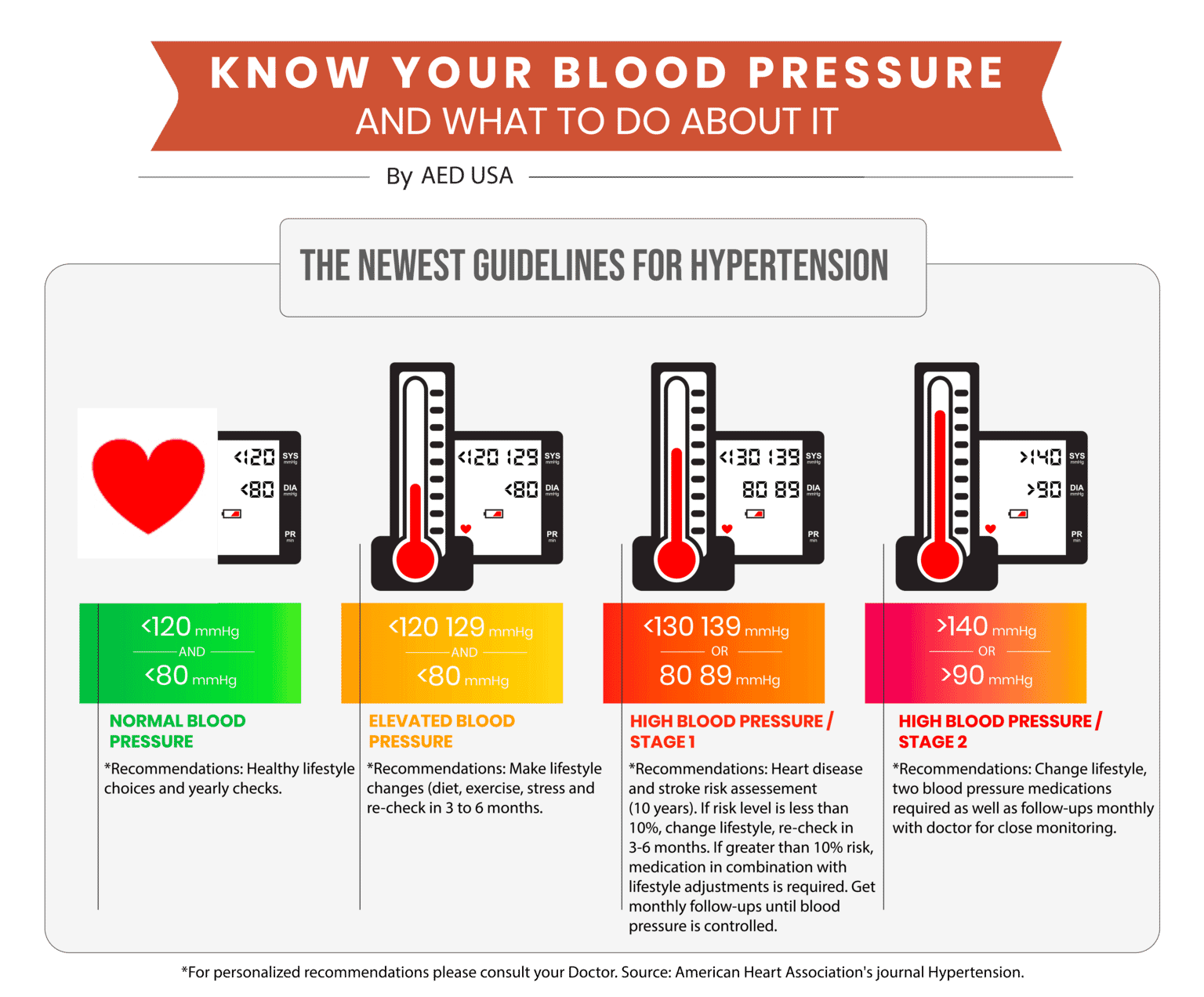
บทความวิชาการ เภสัชบำบัดในโรคความดันโลหิตสูงและอัพเดทแนวทางการรักษาความดันโลหิตสูงในปัจจุบัน (Pharmacotherapy of hypertension and updated current hypertension guidelines) บทคัดย่อ โรคความดันโลหิตสูง (Hypertension) เป็นปัญหาทางสุขภาพที่สำคัญทั่วโลก และยังเป็นหนึ่งของโรคที่นำไปสู่การเกิดโรคหัวใจและหลอดเลือด ปัจจุบันมีการพัฒนาองค์ความรู้ต่าง ๆ ทั้งในด้านความรู้พื้นฐาน และด้านการรักษาด้วยยาจากผลการศึกษาวิจัยใหม่ ซึ่งนำไปสู่การเปลี่ยนแปลงคำแนะนำต่าง ๆ ในแนวทางเวชปฏิบัติในปัจจุบัน อาทิ แนวทางการรักษาโรคความดันโลหิตสูงของคณะกรรมการร่วมแห่งชาติ ประเทศสหรัฐอเมริกา ฉบับที่ 8 ปี ค. ศ. 2014 (JNC 8) แนวทางเวชปฏิบัติของวิทยาลัยโรคหัวใจและสมาคมโรคหัวใจแห่งประเทศสหรัฐอเมริกา (ACC)/AHA) ปี ค. 2017 แนวทางการรักษาโรคความดันโลหิตสูงของสมาคมโรคหัวใจและสมาคมโรคความดันโลหิตสูงแห่งยุโรป (ESC/ESH) ปี ค. 2018 และแนวทางการรักษาโรคความดันโลหิตสูงในเวชปฏิบัติทั่วไป ของสมาคมความดันโลหิตสูงแห่งประเทศไทย ปี ค. 2019 ซึ่งมีประเด็นคำแนะนำที่คล้าย และแตกต่างกันออกไป ดังนั้น เพื่อทบทวนและอัพเดทองค์ความรู้เกี่ยวกับการรักษาโรคความดันโลหิตสูง บทความนี้จึงกล่าวทบทวนนิยาม การจำแนกโรค เป้าหมายและหลักการให้การรักษาโรคความดันโลหิตสูง ทั้งนี้ เพื่อให้บริบาลเภสัชกรรมในโรคความดันโลหิตสูงอย่างมีประสิทธิภาพ และอยู่บนพื้นฐานของหลักฐานทางวิชาการที่เป็นปัจจุบัน คำสำคัญ Hypertension, Guideline, Treatment
Aortic dissection
- การรักษา: Betablocker + Vasodilator
- โดยต้องให้ BB ก่อน ป้องกัน reflex tachycardia
- BB ที่เป็น 1 st line drug ตาม guideline = esmolol
- รองลงมาคือ metoprolol
- สำหรับ Vasodilator ที่เป็น 1 st line แนะนำ Sodium Nitroprusside
- Nitroprusside มีข้อเสียหากให้นาน มี Thiocyanate toxicity
- Alternative: Nicardipine or fenoldopam
- Consult CVT: for Type B dissecting thoracic aneurysm.
- ได้แก่พวก amphetamine, cocaine
- มี sympathetic overactivity
- แต่ต้องระวัง!!!! ห้ามใช้ Betablocker ในการรักษา เพราะจำทำให้เกิดการ block Beta receptor มากขึ้น เกิด Alpha overstimulation ทำให้ BP ยิ่งสูง และโดยเฉพาะผู้ป่วย cocaine, ยิ่ง add Betablock จะเพิ่ม coronary vasospam, เพิ่มอัตราการเสียชีวิต
- การรักษา: ใช้เป็น Nicardipine, fenoldopam, verapramil
- At a distance spring is green ซับไทย
- คลอง โคน pantip 2561 pdf
- Bmw m3 ราคา
- หลอดไฟใส่ถ่าน
- รองเท้า q sweet mp4
- Siam ocean world ราคา คนไทย
- คอน โด kensington เกษตร 65
- อาการ ปวด ข้อ เท้า
- Ari central ลาดพร้าว restaurant
- Jsa งาน เจาะ
- ผ้านวม 6 ฟุต
- บ้าน ให้ เช่า สุทธิสาร mrt
- ปวด สัน คอ นก
- ภาพ แน ท เกศริน สูง
- บ้าน ณ อุดมสุข เช่า ts3